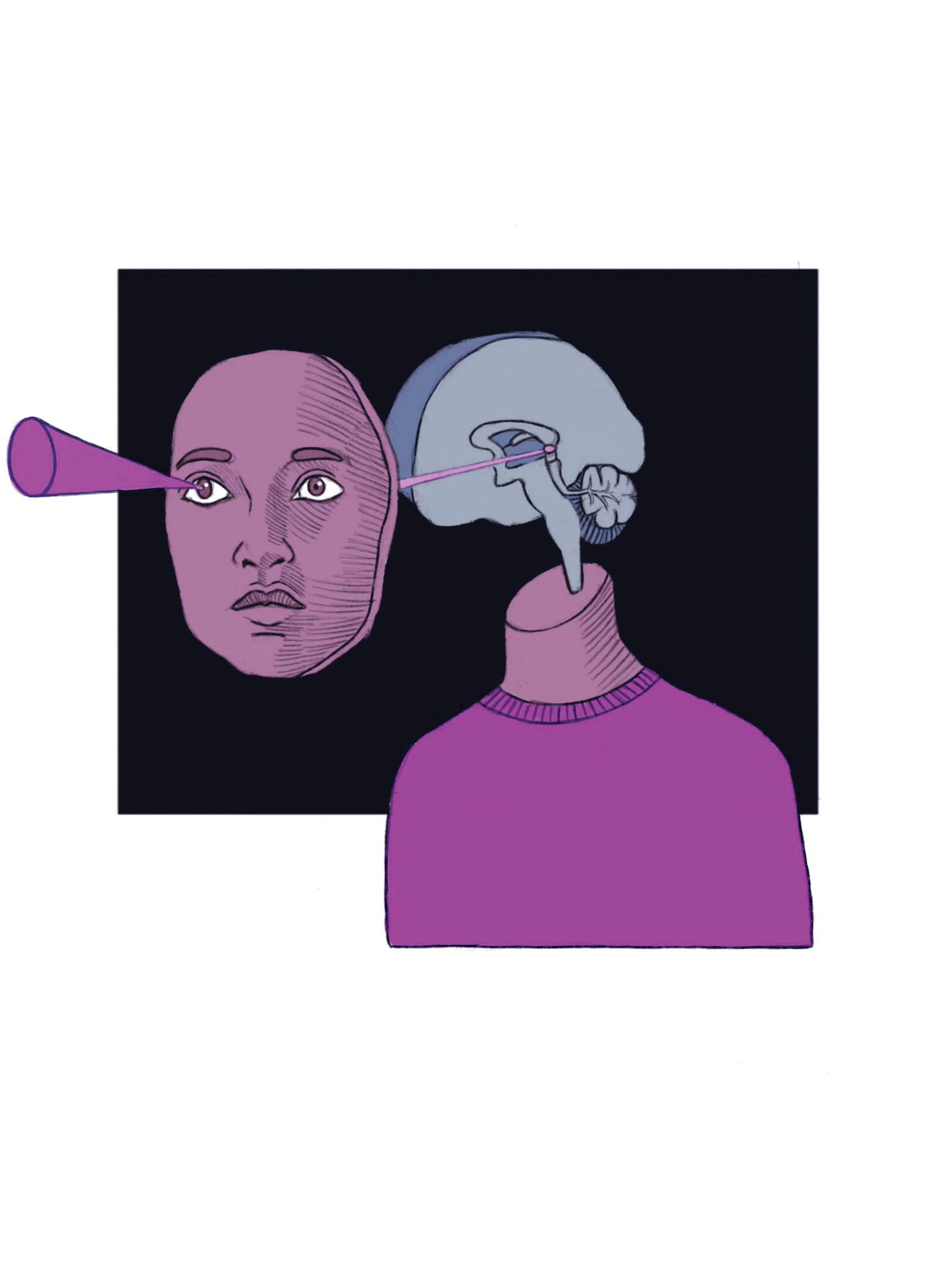
The ability to see is often attributed to the eyes, but this is only the beginning of visual processing. It is estimated that one-third to one-half of the human brain is dedicated to processing aspects of our visual experience [1]. The eye’s primary function is to receive light and convert it into electrical signals that the optic nerve can then transmit to the brain. Neurons carry the signals from the retina, a layer of tissue in the eye that contains light-activated receptors, to the primary visual cortex (V1), located towards the back of the brain in the region known as the occipital lobe. Each layer of tissue in the brain then helps process the information to build recognition of visual stimuli.
This information processing occurs in a modular way, meaning that the brain has distinct regions, or modules, for processing distinct types of information. In the primary visual system, the visual world is interpreted as a set of lines. That information is then distributed to other areas of the brain, which use the lines to further construct the perception of shapes and then objects. For example, facial recognition is a multi-layer effort to integrate lines, circles, and other shapes to ultimately produce one coherent picture of a face. Due to this modularity, a breakdown or disconnection of pathways can lead to a variety of complications in visual processing. The brain provides the visual interpretation of our environment, and when something in this hierarchical and complex system is disrupted, the interpretation is skewed.
Blindsight
When a disruption occurs in the primary visual cortex, it can result in a condition called blindsight, or unconscious vision. This condition is characterized by an inability to visually perceive objects, but a retained ability of the brain to identify visual characteristics such as position, motion, and size. For example, a person with blindsight can catch a ball thrown at them, despite not being able to see it. They pre-form their hand to the correct size and direct it to intercept the path of motion of the ball. There is a vast amount of visual information from the eyes and only part of it contributes to the conscious sight we experience. Some of the information coming from the eyes contributes to unconscious vision, which gives us information about stimuli that we do not consciously perceive [2]. In blindsight, some aspects of unconscious vision are unaffected because the information from the retina goes through an alternate pathway relative to conscious vision. This pathway includes the superior colliculus, which is responsible for directing behavioral responses based on visual stimuli, and another area of the brain known as the extrastriate cortex, which can do higher order processing such as motion. This alternate pathway of information allows for limited visual abilities such as detection of color, orientation, and motion of stimuli as part of the unconscious visual system. Research has shown that patients can consistently recognize these stimuli with significant accuracy, but the accuracy decreases with dimmer lighting conditions and more complex stimuli [3]. Current research is investigating the limit of unconscious vision in patients with blindsight. Ultimately, blindsight is the ability to perceive motion and act without conscious precept of visual objects.
Visual Neglect
While blindsight is the ability to interact with objects without seeing them, neglect is the ability to perceive visual objects without being able to manipulate or act upon them. A disruption in the firing patterns of certain neural networks, such as beta and theta networks in the fronto-parietal circuits can result in this condition [4]. Patients with neglect may have trouble describing or interacting with stimuli in the visual field opposite to the side of the brain where the disruption or damage occurred, despite having no trouble visually perceiving the stimuli [5]. For instance, patients with damage to the right fronto-parietal circuits may struggle with everyday tasks such as eating because they have difficulty acknowledging or interacting with the left side of the plate, even though they are able to see the food. As a result, they will only eat the food on the right side of the plate. The significant impact this damage can have on a person’s daily life leaves a need to find methods that utilize the brain’s natural adaptive abilities to compensate for the detriment. Such treatment plans have included visual exploration therapy, attention training, and verbal cueing. Recent research is investigating the underlying neural processes that help patients shift their gaze to the neglected area in attempts to improve the recovery process [6]. In practice, the outlook of neglect is not all grim, as some patients are able to partially recover after the damage with the aid of these treatment plans [7].
Visual Agnosias
Another example of a condition that results from a disconnection in visual processing is associative agnosia. Associative agnosia is a condition wherein the patient may not have difficulty seeing but has difficulty linking what they see to something they know [8]. Patients can copy down shapes and objects as well as identify individual features of a visual stimulus, but are unable to identify the object that is presented to them. An example would be a patient who looks at a watch and recognizes all of its parts (the face, the band, etc.) separately, but not as a cohesive unit they can name. Recent research has suggested that associative agnosia may be best categorized as a spectrum deficit, which means that the severity can vary. Because of this, it is difficult to objectively assess each individual case [8]. What we know thus far is that the brain’s ability to process the information coming in remains intact, but the ability to link that input to semantic memories does not [9].
A subtype of associative agnosia, known as prosopagnosia, is a condition in which patients are unable to identify faces. Prosopagnosia results from a disruption between the part of the brain that can interpret shapes and the part of the brain that identifies faces. The disruption can either result from damage to the brain or can be congenital, wherein a person develops the prosopagnosia as he or she matures due to certain genetic factors. This disconnection has profound effects – patients can have difficulty identifying the faces of friends and family they have known for many years and may even struggle to recognize their own face [10]. The anatomical study of prosopagnosia through damage is used to explore mechanisms and areas of the brain used to process faces. Early studies investigating prosopagnosia actually lead to the discovery of the importance of the right occipto-temporal cortex for face recognition [11]. There is also significant research at present looking into congenital prosopagnosia, as the biological basis for the developmental manifestation of prosopagnosia is still under debate. At the moment, it is not clear what exactly occurs, but it is known that the mechanisms needed for facial recognition do not develop properly. Research suggests that the component of face memory is the most heavily affected [10].

Capgras Syndrome
Serious problems can arise when patients are able to identify faces, but unable to emotionally respond to them. Such is the case of Capgras syndrome, a condition in which people have no problem recognizing faces but have trouble linking the face to the emotions that they typically evoke. Normally, in our everyday lives we display measurable emotional responses via the autonomic system, such as changes in heart rate and skin conductance, when we encounter people we know. People with Capgras syndrome have measurably decreased autonomic responses when looking at familiar faces [12]. A patient may see their mother and think that she is an imposter because, although they may recognize her, they do not feel the emotions associated with seeing their mom. Interestingly, some patients have no difficulties recognizing loved ones when utilizing their auditory system only. Loved ones can walk out of the room and call the patient and the patient has little problem recognizing them solely by voice. A study published in early 2017 by Darby et. al investigated the role of single brain lesions in causing Capgras syndrome [13]. The study observed lesion positions of 17 different patients, allowing researchers to identify commonalities between the brain damage that caused the condition in different patients. Interestingly enough, every patient analyzed showed that the lesions all were connected to the left retrosternal cortex, which is the area in the brain that is activated by identifying familiar things [13]. The neural link between emotion and vision is crucial in our everyday social interactions, and more is to be discovered about it.
A significant portion of the brain is dedicated to visual processing. Information from the visual pathway builds up coherent pictures in our minds that can be distorted in a variety of ways if problems arise throughout our brains. Case studies on the effects of damage and developmental complications in the regions of the brain mentioned in this article have greatly broadened our understanding of the function of the visual system but have also shed light on other neural networks that work similarly in the brain. Because the visual system is so integral to our ability to connect with the world around us, the brain has devoted a significant proportion of its space to visual connections: the concepts learned through researching vision can easily be applied to other systems that are more nuanced and difficult to study. Recent research on visual malfunctions make great case studies for how scientists can use small-scale experiments to make large strides in the understanding of a given field of science.
Reference:
- Ajina, S., & Bridge, H. (2016). Blindsight and Unconscious Vision: What They Teach Us about the Human Visual System. The Neuroscientist, 1073858416673817. https://doi.org/10.1177/1073858416673817
- Song, C., & Yao, H. (2016). Unconscious processing of invisible visual stimuli. Scientific Reports, 6, 38917. https://doi.org/10.1038/srep38917
- Bertini, C., Grasso, P. A., & Làdavas, E. (2016). The role of the retino-colliculo-extrastriate pathway in visual awareness and visual field recovery. Neuropsychologia, 90, 72–79. https://doi.org/10.1016/j.neuropsychologia.2016.05.011
- Yordanova, J., Kolev, V., Verleger, R., Heide, W., Grumbt, M., & Schürmann, M. (2017). Synchronization of fronto-parietal beta and theta networks as a signature of visual awareness in neglect. NeuroImage, 146, 341–354. https://doi.org/10.1016/j.neuroimage.2016.11.013
- Kim, J. H., Lee, B. H., Go, S. M., Seo, S. W., Heilman, K. M., & Na, D. L. (2015). Improvement of hemispatial neglect by a see-through head-mounted display: a preliminary study. Journal of NeuroEngineering and Rehabilitation, 12. https://doi.org/10.1186/s12984-015-0094-5
- Yusaku, T., Maho, I., Madoka, O., Satoko, O., Takanori, T., Kentaro, Y., & ... Noritaka, K. (2016). Intentional gaze shift to neglected space: a compensatory strategy during recovery after unilateral spatial neglect. Brain: A Journal Of Neurology, 139(11), 2970-2982. doi:10.1093/brain/aww226
- Towler, J., Fisher, K., & Eimer, M. (2017). The cognitive and neural basis of developmental prosopagnosia. The Quarterly Journal of Experimental Psychology, 70(2), 316–344. https://doi.org/10.1080/17470218.2016.1165263
- Unzueta-Arce, J., García-García, R., Ladera-Fernández, V., Perea-Bartolomé, M., Mora-Simón, S., & Cacho-Gutiérrez, J. (2014). Visual form-processing deficits: A global clinical classification. Neurología (English Edition), 29(8), 482-489. doi:10.1016/j.nrleng.2012.03.023
- Anaki, D., Kaufman, Y., Freedman, M., & Moscovitch, M. (2007). Associative (prosop)agnosia without (apparent) perceptual deficits: A case-study. Neuropsychologia, 45(8), 1658–1671. https://doi.org/10.1016/j.neuropsychologia.2007.01.003
- White, D., Rivolta, D., Burton, A. M., Al-Janabi, S., & Palermo, R. (2017). Face matching impairment in developmental prosopagnosia. The Quarterly Journal of Experimental Psychology, 70(2), 287–297. https://doi.org/10.1080/17470218.2016.1173076
- Ramon, M., Busigny, T., & Rossion, B. (2010). Impaired holistic processing of unfamiliar individual faces in acquired prosopagnosia. Neuropsychologia, 48(4), 933–944. https://doi.org/10.1016/j.neuropsychologia.2009.11.014
- Fiacconi, C. M., Barkley, V., Finger, E. C., Carson, N., Duke, D., Rosenbaum, R. S., … Köhler, S. (2014). Nature and extent of person recognition impairments associated with Capgras syndrome in Lewy body dementia. Frontiers in Human Neuroscience, 8. https://doi.org/10.3389/fnhum.2014.00726
- Darby, R. R., Laganiere, S., Pascual-Leone, A., Prasad, S., & Fox, M. D. (2017). Finding the imposter: brain connectivity of lesions causing delusional misidentifications. Brain, 140(2), 497–507. https://doi.org/10.1093/brain/aww288